Do You Want To Beat Endo & Get Your Life Back?
Expert Robotic Surgery and Integrative Support
Endometriosis Healing Re-Imagined
Expert Robotic Surgery
and Integrative Support
Endometriosis Healing Re-Imagined

Our Philosophy = Excision Surgery + Integrative Care !
Diagnostic and expert excision surgery is often a mandatory cornerstone to get you on the right healing path. To start, attention to detail is critical in a proper workup to avoid unnecessary surgery. Before surgery and after, integrative support can make all the difference for rapid recovery. Following that, an integrative Thrivorship program can help long-term outcomes.
FIRST....UNDERSTAND ENDOMETRIOSIS
Extremely common = 1 in 10 women, at least
Extremely under-diagnosed = years of pain & suffering
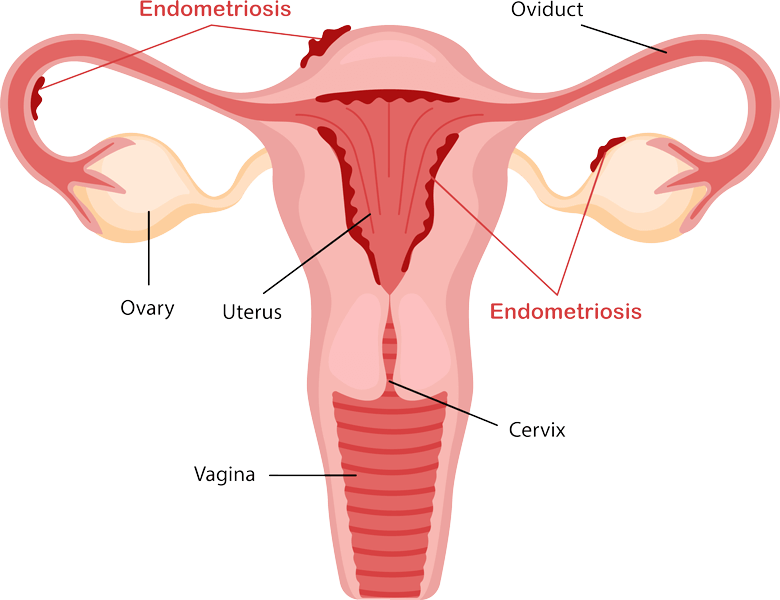
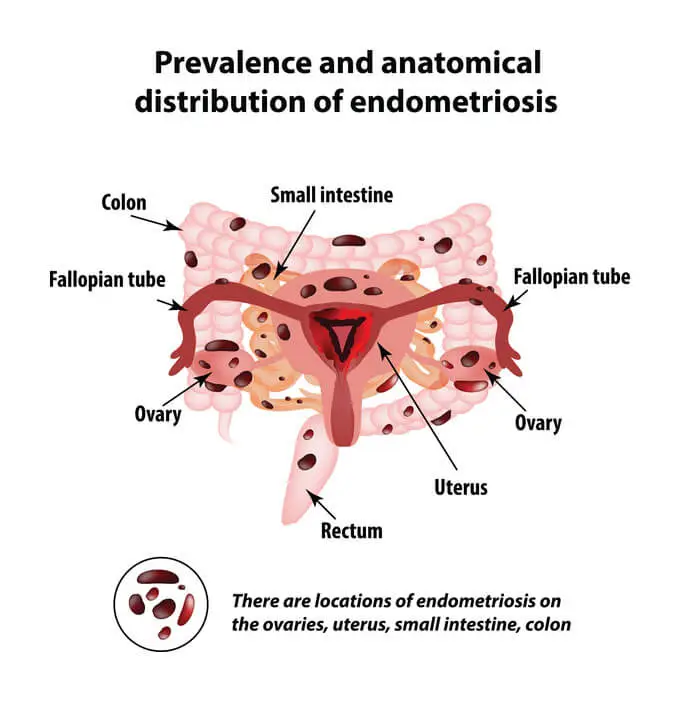
What? Endometrium-like tissue, which is normally inside your uterus, grows abnormally around your ovaries, pelvis, bowel and other organs.
Why? Uncertain and probably differs person to person due to embryologic Müllerianosis, genetics, epigenetics, molecular translational changes, immune factors, retrograde Fallopian tube bleeding specifically of stem cells, pelvic tissue transformation called metaplasia and more. It is most definitely "multi-factorial" and "polygenic".
When? As early as childhood, teens or even earlier in-utero as a fetus. Conversely, can be post-menopausal.
Where? Endo can grow just about anywhere, but most commonly in the pelvis and abdomen.
Symptoms? Pelvic & abdominal pain, bloating, painful sex, infertility, urinary frequency, painful bowel movements, back and leg pain, and FAR more.

ENDO SUBTYPES & SEQUELAE
Superficial endometriosis (on peritoneal surface)
Deep Infiltrating endometriosis (invading tissues)
Ovarian endometriomas ("chocolate cysts")
Metastatic endometriosis (spread to distant areas)
Malignant degeneration (rare but life-threatening)
Endometriosis usually affects pelvic organs and delicate structures nearby, which include your bladder, ureters and rectum. It can move to your abdomen and intestines and, rarely, to many other organs and tissues.
ENDOMETRIOSIS CRITICAL TIP
Get the diagnosis straight and get it right early! Don't “grin and bear it” with your pelvic pain with no answers from your doctor. Get a second opinion. The earlier endometriosis treatment starts, with or without minimally invasive surgery excision, the better the outcomes and the faster you can get back to a good quality of life!
ENDOMETRIOSIS SUMMARY FACTOIDS

Very common yet under-diagnosed
Atypical pain, bloating, silent infertility and many more symptoms
Proactive lifestyle mods
Diet and lifestyle can reduce excess estrogen & produce other molecular signals that may reduce growth and progression of endometriosis

Integrative holistic support
Endometriosis and symptoms may be reduced by herbals/botanicals and lifestyle modification, which impact specific genetic & molecular pathways.

Diagnosis
Surgical biopsy is the only way to diagnose endometriosis. Imaging and biomarkers MAY help plan treatment.

Treatment
Endo is best treated with a personalized combination of medical and surgical approaches.

Surgical excision
Best surgery for endometriosis is excision of implants using minimally invasive surgery with laparoscopy or robotic surgery.

Master endometriosis surgeons
Not a time for amateur hour at your expense! Ideally, find a master surgeon , or at least an expert, who has advanced minimally invasive and robotic surgery skills and who understands the principles and practice of endometriosis excision. It's critical to your success!
ENDOMETRIOSIS PREVENTION AND DETECTION
YOU may be predisposed with 5 to 7X risk if close relatives have endo.
Molecular genetics is leading to discovery of critical genetic "on/off" switches.
There is no preventive or magic medicine but with integrative holistic attention to your body, your nutrition, your lifestyle, your exercise habits and key botanicals MAY help fight endo by interacting with these molecular processes. This may also reduce cancer risk, which is slightly higher in women with endo.
DOES EXERCISE HELP PREVENT & CONTROL ENDO?
Hit it with HIIT. "High intensity interval" or "burst training" means best BMI, more lean muscle mass and increased human growth hormone (HGH).
Normal percentage body fat (lower BMI) means a lean fat burning machine which, in turn, means less excess estrogen. But don't overdo it, very low BMI can increase risk of endo. It's complicated.
CAN A SPECIAL DIET HELP BEAT ENDO?
Make veggies the “base” of your diet, meaning "whole food plant-based"......not sugar-laden junk food!
Losing weight means less fat. Fat makes & stores estrogen. Decrease it!
Regular longer cycles, less estrogen, means less endo stimulation.
Maintaining healthy fiber and probiotics in your diet also helps digest, bind and flush excess estrogen.

In this video actress Tia Mowry explains endometriosis, and how dietary changes helped her. Consider doing it.
DOES DRINKING ALCOHOL AFFECT ENDO?
Alcohol causes estrogen spikes in your body which can feed endo growth. It can also make you fat, which also feeds endo. So, cut the drinking down.
DOES COFFEE MAKE ENDO GROW?
Consuming caffeinated drinks can also cause estrogen levels to rise and stimulates the bladder, worsening interstitial cystitis (co-exists with endo).
Seek less caffeinated solutions like some teas, which also contain other healthy phytonutrients.
HOW DO XENOESTROGENS MAKE THINGS WORSE?
What's that !? It's part of all that stuff you put on or in your body!
Toxins are all around.....you're exposed to ~30,000 per year.
These are hormone-like endocrine disruptors and store in your fat cells.
Where are these coming from? Long list! Processed meat and dairy, insecticides, unfiltered tap water, food additives, hair and skin products, even toothpaste. Learn more: EWG.org
AVOID SOY?
No! If you're worried about the GMO part, buy organic or grow your own.
Soy isoflavones mainly block standard estrogen at the receptor level.
This means less potential stimulation of endometriosis cells.
CAN SEAWEED HELP?
Seaweeds, like bladderwrack, may gently lower estrogen levels.
500-700mg a day will do it.
More is not "better", because of iodine content....good in moderation.
Japanese women, on a traditional local diet, have among the lowest rates of breast, endometrial, and ovarian cancers, as well as longer menstrual cycles and lower estrogen levels circulating in their blood.
ENDOMETRIOSIS DIAGNOSIS
SURGERY & BIOPSIES OR SCANS?
In short, surgery with biopsies is the only way to diagnose endo.
Imaging scans (Ultrasound, CT, MRI) can only help decide about surgery and extent of surgery that might be needed.
Pain with normal scan does NOT mean there is no endometriosis because endo implants can be flat and hard for scans to see.
MRI is best for determining if cysts are likely endometriomas and to look for adenomyosis of the uterus.

ARE THERE ENDOMETRIOSIS BLOOD TESTS?
Endo is bio-inflammatory, so biomarkers like hsCRP and CA-125 can be elevated.... but any inflammation can cause elevation.
"Omics" is the almost-here future! Genomics, metabolomics, proteomics can all spawn diagnostic tests
MicroRNA (miRNA) signatures are being studied in our research lab and others, and some are in clinical trials for diagnosis, monitoring and treatment of endo.
ENDOMETRIOSIS TREATMENT
Treatment of endometriosis is partly dependent on where it is located (pelvis or outside the pelvis) and what the stage is. Staging is a classification of the severity of pelvic endo.
WHAT ARE ENDOMETRIOSIS "STAGES"?
According to ASRM (American Society for Reproductive Medicine), there are four stages of pelvic endometriosis. Someone can have high stage and less pain than another person with lower stage and more pain. This should give you the general idea about how this is categorized, but there are other staging systems.

STAGE I
MINIMAL ENDOMETRIOSIS
There are small patches or implants either on or around the organs in the pelvis.
STAGE II
MILD ENDOMETRIOSIS
There are more implants than in Stage I but damage to the pelvic organs is still pretty minimal and there’s not much scarring or adhesions. Altogether, when summed up the implants are not more than 5cm (couple of inches).

STAGE III
MODERATE ENDOMETRIOSIS
Implants are more widespread and are beginning to infiltrate (grow into or invade) the organs in the pelvic region, including pelvic side walls (where the blood vessels, major nerves and ureters are located) and peritoneum. There is more scarring and adhesions and endometriomas (“chocolate cyts”) on the ovary.
STAGE IV
SEVERE ENDOMETRIOSIS
The disease is definitely infiltrating or growing into and affecting several organs in the pelvic region as well as the ovaries. This may be the bladder or the rectum. Anatomy is severely distorted with scars and adhesions and there is fibrosis (like concrete) between organs. Larger and more endometriomas can be seen.
ENDOMETRIOSIS SURGICAL TREATMENT
Why is surgery helpful for endometriosis? TWO reasons:
Definitive biopsy diagnosis of endometriosis
Cornerstone excisional treatment of endometriosis
Earlier excision may mean more pain-free years for you and less organ damage from scarring and fibrosis.
Less scarring means enhanced chances for fertility.
Individualized surgical planning is crucial for best results.

WHAT TYPE OF SURGEON FOR ENDOMETRIOSIS?

The more endo you might have, the more you need a master surgeon and not a dabbler. For sure you need an über master surgeon if repeat surgery is needed.
How do you know how much endo you have? That's often not possible to tell until surgery. This is why you should find the best and highest level expert you can to help you, always !
The following is what you get for each level of training:
General ObGyn surgeon: Formal 4yr residency leads to board certification and surgical skills for diagnosis and benign basic ovarian and uterine surgery ; often fulgurate/ablate endo rather than excise; not trained in retroperitoneal surgery; very limited abilities on bowel, ureters and abdominal organs. Usually don't study endometriosis in depth.
Endo Excision surgeon: Additional informal 1-2yr fellowship not leading to second board certification for minimally invasive endo excision and endometriosis management; usually work with a team including gynecologic oncology, general surgery and/or urology for bowel and urinary tract surgery. Significant added expertise in endo management, but depends on fellowship.
Gynecologic oncologist: Additional formal 3-4yr fellowship in complex pelvic surgery, focusing on cancer and a second board certification; this master surgeon is at the pinnacle of gynecologic surgical expertise; best equipped if distorted anatomy and for handling bowel, rectum, ureters, bladder and all abdominal organs up to and including the diaphragm; most do not study endometriosis in detail; some are not minimally invasive.
So, when should a “cancer surgeon”, a gynecologic oncologist, possibly be involved in YOUR endometriosis treatment? First, gynecologic oncologists have an advanced skill set to operate not only on gynecologic organs but also on surrounding intestine, rectum, ureters and bladder; all of which can be affected with endometriosis in advanced cases, including repeat surgeries which usually have more scarring present. Second, as you get older, endometriosis is associated with an increased risk of ovarian cancer as well as degeneration of endometriosis itself to clear cell cancer or sarcoma. These are things you do not want missed and are especially important to be evaluated for as you get older with a diagnosis of endometriosis. Whether or not these surgeons should be your primary endo excision expert depends on whether or not they focus on endo.
Consulting Surgeon Qualifications:
In addition to the above, a team may include a general, thoracic, urologic, vascular and neurosurgeon, depending on the problem at hand. Usually fewer consultants are required if a gynecologic oncologist is involved because they can perform most of all that is required.
If your main concern is about fertility issues with a diagnosis of endometriosis, a reproductive endocrinologist’s opinion would be very helpful. A few still participate surgically and specialize in endo.
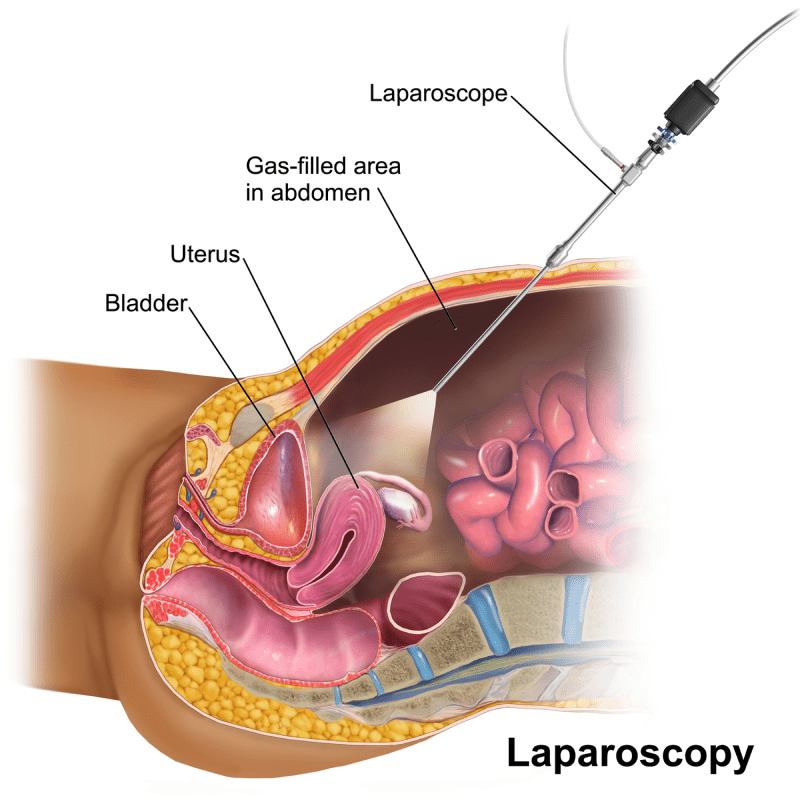
MINIMALLY INVASIVE SURGERY
Laparoscopic Excision
The original "keyhole" or "belly button" surgery
5mm incision around belly button and 2-4 additional incisions
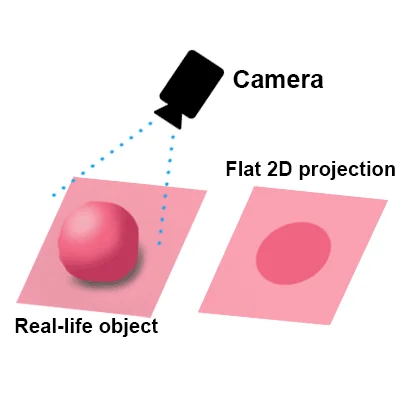
2-Dimensional camera (no depth perception; like operating with one eye closed)
Instruments are "straight sticks" with graspers and scissors at the tips. Push, pull, cut, tear....so can be traumatic and lacks finesse.
So...laparoscopy is better than big open incision surgery (laparotomy), it's "ok" for "basic" cases with a good surgeon, but it's oh so yesterday....
Q: How do we know if a case is "basic" before the surgery happens?
A: We don't.... that's the problem.
BOTTOM LINE: For more advanced surgery not having that visual magnified 3-D third dimension is like operating with one eye closed. You lose the depth perception that is very important for delicate surgery in difficult spaces. Try closing one eye and doing things around the house, picking things up, and so on. It’s harder to do isn’t it?
You can certainly compensate, as people do when they lose an eye, but it’s harder to judge what is further from or closer to you. So, given a choice, using both eyes is better and 2-D laparoscopy screens mimic having one eye closed. This is part of why robotic surgery adds safety to endometriosis excision.
Robotic Surgery Excision
21st Century endo excision tool of choice. Period! Why?
Robotics is laparoscopy "on steroids" because:
3-D magnified high definition camera for ultimate depth perception and magnification on demand
Instruments that are "wristed" making them like tiny human hands holding scissors and graspers.
Advanced artificial intelligence and programming limits any jittery moves a surgeon may make, smoothing it all out.
This means:
Less trauma and tissue injury internally due to finesse "wristed" instruments
Less blood loss because of the precise instruments and better visibility
Less trauma to your abdominal wall because the instruments do not move as much as with laparoscopy

THESE FEATURES LEAD TO:
Shortest possible recovery time
Less pain
Fewer complications, transfusions and readmissions
Very rare “conversions” to a big incision due to inability to finish the surgery via minimally invasive approach
Better ability of surgeon to fully excise endometriosis even in hard to get to areas
BOTTOM LINE: Robotic surgery is based on far superior technology, both the 3-D high definition magnified optics and the instruments. This all but guarantees safer surgery, even for complex high stage or recurrent endo.
But......it's not the robot that is operating. It's the surgeon. Many surgeons have completed basic robotic surgery training, but you do not want a rookie surgeon for complex endo surgery. You don't even want one that does this some of the time. Select wisely, and go with a master surgeon that devotes all of their time to endo excision and even more complex gynecologic surgery.

MEDICAL TREATMENT
Medical endometriosis treatment is largely based on hormonal options and/or pain symptom management. At this time we focus on what we do best, which is our very specialized and advanced surgical help, as well as counseling about cancer risk.
In most cases, especially if you are out of area, we will advise you and collaborate with your gynecologist or reproductive endocrinologist but do not provide extended hormonal therapy for endometriosis. If you do not have someone that can manage the medical and hormonal part of your endo care, we can help you find someone to be part of your local endometriosis-fighting team!
HERBAL & BOTANICAL SUPPORT
For symptoms of endometriosis, as well as potential epigenetic and molecular impact on endometriosis growth drivers, there are many integrative natural support options to consider and here is an example of just a few:
TURMERIC
This spice contains a bioactive ingredient called curcumin, which is a strong anti-inflammatory. Pepper helps its absorption. It’s best to use the root or spice and just add to your salads or as part of curry dishes.

GINGER
This natural root also reduces inflammation and helps reduce nausea that may be caused by the pain of endometriosis. You can make ginger tea by boiling 1 tablespoon of grated ginger into 2 cups of water for 10 minutes. After straining it, add honey. You can also get some ginger pieces and simply chew on them as needed.

CHAMOMILE
This natural herb from daisy-like flowers is also an anti-inflammatory. But beware that it is also a diuretic, so it can make you feel the urge to pee often. You can make chamomile tea by steeping 2 teaspoons of dried chamomile mix in 1 cup of hot water for five minutes, straining it and adding honey for sweetness if desired. Chamomile supplement capsules also exist if it’s inconvenient to make tea.

BROMELAIN
Bromelain is an enzyme which helps digest protein and has been used as a digestive aid and anti-inflammatory agent. It can be taken in capsule form, but fresh pineapple pulp is a great source. It can help in postoperative healing with minimal scarring.
ENDOMETRIOSIS TREATMENT OUTCOMES

CAN ENDOMETRIOSIS BE CURED?
The standard answer to this is "no", because it is difficult to cure any disease when the exact cause is unknown. Such is the case with endometriosis.
But, as we enter the molecular age of targeted therapy, this will change. However, today, anyone with endometriosis is at risk for recurrence at some point, after any medical or surgical therapy. Better surgery and comprehensive integrative treatment may lead to lower recurrence rates.
So, the best plan is to make sure the diagnosis is correct, removal of significant disease with minimally invasive surgery (especially deep infiltrating endo and endometriomas), then focus on ways to minimize estrogen excess in your body and other drivers of endo growth. This may include medical treatments listed above or simply being as fit, lean and xeno-toxin free as you can be.
Sometimes, repeat surgery is required, but you want to limit the number of times this is done to limit scarring from the surgery itself, which can also produce pain. Also, the more surgeries are performed and the more scarring (adhesions) that are potentially created, the more complications are increased. Working with a master surgeon is crucial to reducing the need for repeat surgery(ies).
LOOKING BEYOND LIFE WITH ENDO
After a head start with an optimal master surgeon endo-excision, integrative perioperative healing: mind, body, spirit rounds out recovery.
Thrive with guidance for long-term customized strategies....
So, you can be you !
STEVEN A. VASILEV MD BIOGRAPHY
“I help and guide women to defeat endometriosis, gynecologic cancers, and complex gynecologic conditions using a unique combination of minimally invasive robotic surgery, precision cancer therapies and complementary holistic natural support towards thriving in survivorship.”
Dr. Vasilev is the only physician triple board certified in Ob-Gyn, Gynecologic Oncology and Integrative & Holistic Medicine in the United States. He is an accomplished world-renowned oncologic and robotic surgeon and has trained hundreds of fellows and residents. He served as the inaugural Medical Director of Integrative Medicine for seven years and is Co-Chair of Robotic Surgery at Providence Saint John’s Health Center, Professor at Saint John’s Cancer Institute in Santa Monica, California and is Clinical Professor at Loma Linda University School of Medicine.
His residency and fellowship, leading to two of his three board certifications (ABOG/ABMS), included extensive training in surgery not only on gynecologic organs but also bowel, bladder, ureters, diaphragms and all other organs in the abdomen and pelvis that can be affected by cancer, endometriosis and related conditions. This, combined with over three decades of experience in advanced minimally invasive surgery, allow him to safely complete very advanced surgeries.
Since completion of his fellowship training in Gynecologic Oncology at the USC Kenneth Norris Comprehensive Cancer Center he has been recognized as a surgical innovator, minimally invasive surgery pioneer (among first group in the US to regularly perform complex laparoscopic surgery such as radical hysterectomy and lymph node dissection in the late 80’s and early 90’s), and thought leader. He has held multiple leadership positions and been on the faculties of Kaiser Permanente, City of Hope, UC Irvine, USC, UCLA and Loma Linda University.
Dr. Vasilev has lifelong experience and training in integrative holistic medicine and is also board certified in that speciality by ABOIM (ABPS).
Dr. Vasilev has been involved in running research programs at multiple sites since 1977. He is a sought-after speaker, has authored over 90 publications, abstracts, book chapters and is the author-editor of a gynecologic oncology textbook and several popular books on integrative oncology and ovarian cysts.
DR STEVE VASILEV’S RESEARCH, PUBLICATIONS & BOOKS


Dr Vasilev is extensively published and according to Academia.edu his work has been cited by other professionals and colleagues hundreds of times, meaning he is a respected national expert on multiple topics related to cancer, minimally invasive surgery, peri-operative recovery and integrative medicine.
LOCATIONS:
San Luis Obispo
Los Angeles
Beverly Hills
Santa Monica
Marina del Rey
FOCUS:
Endometriosis Excision
Endo Associated Malignancy
Robotic Surgery
Pelvic Masses
Complex Gynecology Surgery
Ovarian Cysts
© Steven Vasilev MD PC | Gynecologic Oncology. All Rights Reserved 2015-2024.